Case Report / Open Access
DOI: 10.31488/bjcr.215
Silicone Bleeding From The Monobloc Hydrogel Saline Breast Implant, A Case Report.
Evert van den Broek1 and Rita Kappel2,*
1. Department of Pathology, University Medical Center Groningen, Groningen, The Netherlands.
2. Plastic and reconstructive surgeon, Dr. Kappel Institute, Zwolle, The Netherlands.
*Corresponding author:Dr. Rita Kappel MD; Ph.D. Dr. Kappel Instituut / Willemskade 14, 8011 AD Zwolle, The Netherlands +31-384225755; E: info@drkappel.nl
Abstract
Silicone breast implants are known to bleed silicone molecules, which can be demonstrated by pathological examination of periprosthetic capsular tissue. Evidence is emerging that this phenomenon may contribute to the development of breast implant illness (BII). To reduce such risks, alternative implants have been developed, including saline-filled devices such as the Monobloc hydrogel implant. However, it remains unclear whether silicone bleeding also occurs in these implants. We describe a case of a woman who received Monobloc hydrogel saline breast implants as her first and only breast prostheses. Sixteen years after implantation, she presented with systemic symptoms consistent with BII and requested explantation. Histopathological examination of the capsular tissue unexpectedly revealed silicone deposits, identified by conventional light microscopy and confirmed by Modified Oil Red O (MORO) staining, despite the absence of silicone gel within the implant. As no alternative source of silicone exposure was present, the elastomer shell of the implant is the most likely origin of these deposits. This case showed that silicone bleeding may also occur in Monobloc hydrogel implants.
Introduction
Since the early 2000s, the Monobloc hydrogel, developed by Henri Arion in France, has been considered a safer alternative for breast augmentation and post-mastectomy reconstruction. Unlike traditional silicone gel–filled implants, the Monobloc device contains a hydrogel composed of 97% saline and 3% carboxymethyl cellulose, a polysaccharide assumed to be biodegradable (1,2). Due to its composition, this implant was believed to minimize health risks associated with silicone exposure. Patients have reported high satisfaction rates, particularly regarding the natural consistency and aesthetic outcomes. Many women received Monobloc hydrogel implants. In a previous study was suggested that replacing silicone gel implants with Monobloc hydrogel implants may reduce symptoms potentially related to breast implants (2). However, little is known about outcomes in patients for whom the Monobloc implant was the primary and only prosthesis. In this report, we describe a case in which capsular tissue from a patient with long-term Monobloc hydrogel implants was examined histologically.
Case description
In 2021, a woman presented to our clinic with health complaints (fatigue, muscle pain, cramps in legs, palpitations, fever attacks and anxiety), which were considered compatible with breast implant illness (BII) (3). Sixteen years ago, she had a breast augmentation with Monobloc hydrogel implants, which were her first and only breast prostheses. Based on her clinical presentation and personal preference, explantation was performed. Both implants were found to be intact. Small capsular tissue biopsies were obtained and investigated by the pathologist as part of routine pathological evaluation. Implant identification details were reported (Monobloc hydrogel, Laboratoire ARION, 210 HP; Lot nr. Right side: 0111633; Lot nr. Left side: 0111536). At three-month follow-up, the patient reported a notable reduction in her symptoms. No additional reconstructive procedures were required.
Tissue examination
Periprosthetic tissue samples were processed according to standard protocols by the pathology department. Standard hematoxylin–eosin stained (HE) slides were performed using formalin-fixed paraffin-embedded (FFPE) material. In addition, a Modified Oil Red O (MORO) stain was performed to confirm presence of silicone material (4). The slides were examined by conventional light microscopy. The use of patient material (FFPE) was in compliance with the Dutch ‘Code for Proper Secondary Use of Human Tissue’ (www.federa.org).
Results
Histological analysis revealed a collagen-rich fibrous capsule. A layer of mononuclear inflammatory cells with macrophages was observed covering the fibrous capsule. Translucent amorphous foreign material was identified, partially located within vacuolated cytoplasm of macrophages on HE staining (Figure 1a). These findings were suggestive of silicone deposits and were confirmed by positive MORO staining (Figure 1b).
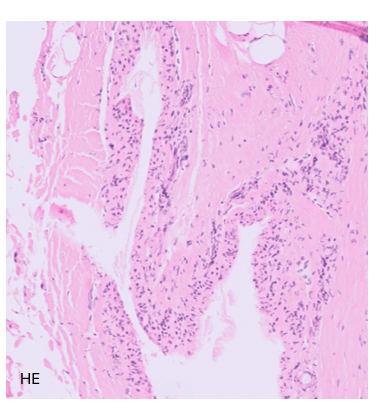
Figure 1a:H&E staining. Translucent amorphous material was identified, partly located within vacuolated macrophage cytoplasm on H&E staining.
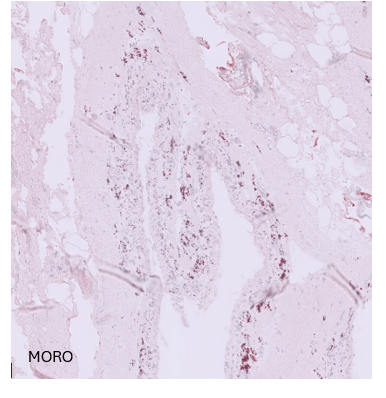
Figure 1b:MORO staining Silicone deposits were confirmed by positive Modified Oil Red O (MORO) staining, which visualizes silicone in a reddish colour
Discussion
At the time of implantation in 2001, Monobloc hydrogel implants were considered a safer alternative to silicone gel implants, based on the assumption that the hydrogel content (saline 97% and 3 % carboxymethyl cellulose) posed minimal health risk and that silicone release from the elastomer shell would be negligible (5-7). In this case, however, the patient developed symptoms consistent with BII, prompting explantation of her implants. Unexpectedly, silicone deposits were identified in the capsular tissue despite the absence of silicone gel within the implant. This finding suggests that the elastomer shell may still release silicone molecules to surrounding tissue. This challenges the assumption that hydrogel implants eliminate the risk of silicone exposure.
Although causality between silicone exposure and systemic symptoms remains debated, this case indicates that silicone bleeding may also occur in non–silicone-filled implants and should not be disregarded in clinical evaluation.
Conclusion
This case demonstrates unexpected presence of silicone deposits in capsular tissue of Monobloc hydrogel saline breast implants. Despite the absence of silicone gel filling, the elastomer shell appears to be a source of silicone release.
References
1. Arion H. Carboxy-methyl cellulose hydrogels used to fill breast implants: 15 years of experience. Ann Chir Plast Esthet. 2001;46:55–59.
2. Kappel RM, Pruijn GJ. The monobloc hydrogel breast implant: Experiences and ideas. Eur J Plast Surg. 2012;35:229–233.
3. Kabir R, Stanton E, Sorenson TJ, et al. Breast implant illness as a clinical entity: A systematic review of the literature. Aesthet Surg J. 2024;44:NP629–NP636.
4. Kappel RM, Boer LL, Dijkman H, et al. Gel bleed and rupture of silicone breast implants investigated by light microscopy, electron microscopy and energy dispersive X-ray analysis of internal organs and nervous tissue. Clin Med Rev Case Rep. 2016;3:1–9.
5. Barker DE, Retsky MI, Schultz S, et al. Bleeding of silicone from bag-gel breast implants and its clinical relation to fibrous capsule reaction. Plast Reconstr Surg. 1978;61:836–841.
6. Beekman W, Feitz R, van Diest PJ, Hage JJ, et al. Migration of silicone through the fibrous capsules of mammary prostheses. Ann Plast Surg. 1997;38:441–445.
7. Smahel J. Foreign material in the capsules around breast prostheses and the cellular reaction to it. Br J Plast Surg. 1979;32:35–42.
Received: February 25, 2026;
Accepted: March 15, 2026;
Published: March 18, 2026
.
To cite this article : Evert van den Broek and Rita Kappe.Silicone Bleeding From The Monobloc Hydrogel Saline Breast Implant, A Case Report. Br J Cancer Res. 2026;9(1):857-858. doi:10.31488/bjcr.215.
© The Author(s) 2026. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/).