Research article / Open Access
DOI: 10.31488/bjcr.211
Symptom Prevalence Among Cancer Patients Attending the Outpatient Palliative Care Clinic: A Single Institutional Experience
Ayman Allam1, Zeinab Idris1, Azza Hassan1,2, Shaikhah Al Keldi1, Hodan Abdullah1*, Saad Jobran1, Aamna Hamid1, Azar Naveen1, Hiba Eltahir1, Sair Ibrahim1, Alaa Khalafalla1, Dr. Afshan Adil1, Dr. Soubiya Ansari1
1. National Center for Cancer Care & Research, Hamad Medical Corporation, Doha, Qatar
2. Weill Cornell Medicine-Qatar, Doha, Qatar
*Corresponding author:Hodan Abdullah, National Center for Cancer Care & Research, Hamad Medical Corporation, Doha, Qatar,Email: HIBrahim7@hamad.qa
Abstract
Introduction: Cancer patients suffer from a variety of distressing symptoms that affect their quality of life. Thus, exploring these symptoms is highly needed. Addressing these symptoms will help to improve their quality of life. Aim: To analyze symptom prevalence among patients with advanced cancer in their initial visits to palliative care clinics. Methods: A descriptive cross-sectional study including 300 cancer patients assessed for symptom prevalence upon their first visit to the palliative care outpatients. The ESAS-r tool was used to evaluate symptom prevalence. Different variables such as age, gender, type of cancer, symptom severity were also studied. Results: The study revealed the 4 most common prevalent symptoms were wellbeing (90%), pain (86%), fatigue (75%), and anxiety (59%). The most common cancer types were breast cancer (21%), Gastrointestinal cancer (20%), hepatobiliary cancer (14%), and lung cancer (12%). Conclusion: Low wellbeing, pain, fatigue, anxiety, and anorexia are the most common prevalent symptoms among cancer patients seen in palliative care outpatients in initial visit.
Keywords: symptom, prevalence, palliative care, outpatients, cancer, inpatient
Introduction
Cancer is a complex and challenging disease that affects both patients and their families. As it progresses, a multitude of distressing symptoms become more prominent and severe, impacting the patient's quality of life. Despite the great advancements in cancer treatment and supportive care measures, numerous patients continue to deal with a variety of distressing symptoms. Thus, understanding the prevalence of said symptoms, specifically in a palliative care population diagnosed with cancer, helps a physician to recognize different effective strategies in improving overall wellbeing, and hence quality of life [1].
Fatigue and pain undoubtedly prove to be the two most common symptoms experienced by cancer patients referred to palliative care services. This is well-proven by a recent study authored by Webber et al. [2], which displays a rate of 89% patients reporting fatigue and 83% reporting pain. Additionally, feelings of drowsiness (77%) and dry mouth (70%) were reported. Among those patients, 31% experienced significant psychological distress, with accompanying anxiety and to a lesser extent depression. Dyspnea, anorexia, nausea, and vomiting were also present in about 40%-50% of palliative care patients.
The Edmonton Symptom Assessment Scale (ESAS) is a widely used, simple and reliable tool for assessing the severity of symptoms experienced by patients with advanced progressive cancer. This tool is frequently used in palliative care and has proven its reproducibility [3]. Its primary objective is to evaluate and monitor symptoms that patients are dealing with, allowing suitable interventions and treatment to improve their quality of life. The ESAS, which is developed in 1991, has undergone improvements over the past 27 years since its inception and has resulted in a modified version now known as the revised ESAS (ESAS-r). The revised scale consists of nine core symptoms: pain, tiredness, nausea, drowsiness, appetite, shortness of breath, depression, anxiety, and feelings of well-being. An additional 10th item was added to document any other additional symptom of particular importance to the patient which is not included in the initial 9 symptoms. Symptom severity is rated on a scale from 0 to 10. Over the years, ESAS-r has evolved to become a pivotal component in symptom gauging patients with advanced cancer in palliative care units and has proved its efficacy.
The primary aim of the present study is to identify the most common prevalent symptoms in palliative care patients attending the Outpatient Clinic Department (OPD) for their first visit. Evaluation of symptoms were carried out using the ESAS-r. Symptom prevalence among said OPD cancer patients referred to palliative care were analyzed, and the severity of each symptom reported. Factors such as age, gender and cancer type were analyzed.
Methods
Study design
The present study is a descriptive cross-sectional study including 300 patients. Those patients,have been newly referred to palliative care outpatient clinics, and previously diagnosed with advanced cancer. Referrals have been done to palliative care outpatient clinics through Medical Oncology and Hematology physicians at the National Center for Cancer Care & Research (NCCCR), which is the only existing hospital for cancer care in the state of Qatar. The patients were recruited between 6th October 2021 to 10th August 2023. Symptom prevalence was assessed for the most common symptoms among cancer patients including that of pain, fatigue, drowsiness, dyspnea, anorexia, nausea and vomiting, anxiety, depression, and well-being. To assess the above given symptoms, the ESAS-r tool was used. The ESAS-r tool has already proven its validity and reproducibility [3], Which allowed be widely accepted in numerous centers for the initial evaluation of cancer patients receiving palliative care. Variables such as age, gender, cancer type, and symptom severity have been assessed in this study.
Sample size
The sample size for this study was determined based on the prevalence of the least common symptom on the (ESAS-r) tool. According to prior research by Rajvi S. et al. [4], the prevalence of nausea was reported to be 28%. Using the single proportion formula with a 95% confidence level and a 5% margin of error, the required sample size was calculated to be 310 participants. A total of 300 participants completed the ESAS-r assessment. Although slightly below the target, this sample size still provides sufficient statistical power to estimate symptom prevalence with acceptable precision. A convenient sampling method was used to recruit participants for this study. This non-probability sampling approach involves selecting participants who are readily accessible and willing to participate. Eligible patients who were present at the data collection sites during the study period and met the inclusion criteria were approached consecutively and completed the ESAS-r assessment.
The ESAS-r tool was performed for each patient either by the palliative care Clinical Nurse Specialist , the Palliative Care Physician or the patient during his/her first visit to the outpatient palliative care clinic as a part of the initial comprehensive palliative care assessment. Inclusion criteria included patients ≥ 14 years with cancer diagnosis and seen for the first time in the palliative care outpatient clinic. Patients < 14 years of age, with non-cancer diagnosis or seen for the first time by palliative care team outside the outpatient clinic, such as inpatient consultation to palliative care, or previously seen in the outpatient clinic were excluded.
Statistical analysis
Multiple techniques were used to ensure the integrity and validity of each variable. Missing values were examined, and a descriptive analysis was conducted. The categorical variables are presented as percentages, while the continuous variables are summarized with mean values, standard deviations, and medians when appropriate. Additionally, a chi-squared test was used to assess the symptoms in relation to different age groups that has been categorized as (< 65 years, and ≥ 65 years). The significance level was established at P <0.05. All statistical analyses were carried out using STATA 15 (Stata Corporation, College station, TX, USA). The chart is produced using Microsoft Excel.
Results
The present study included a total of 300 patients who were comprehensively assessed for symptom prevalence, using the ESAS-r tool at their first visit to the palliative care outpatient clinic. The study was carried out in the period from October 2021 to August 2023. There were 156 males (52%) and 144 (48%) females; the mean age of included patients was 54 years, ranging from 17 to 94 years. The 4 most common cancer types encountered were breast cancer (21%), followed by Gastrointestinal cancer (20%), hepatobiliary cancer (14%), and lung cancer (12%), as displayed below in Table 1.
Table 1. Patients’ Characteristics
| Variable | Statistics n =300 |
|---|---|
| Age by years Mean ( | 54.6 (12.9) |
| Range | 17 - 94 |
| Gender N (%) | |
| Male | 156 (52.0%) |
| Female | 144 (48.0%) |
| Type of cancer N (%) | |
| Brain | 4 (1.3%) |
| Breast | 62 (20.7%) |
| GI | 61 (20.3%) |
| Gynecology | 34 (11.3%) |
| Head and Neck | 17 (5.7%) |
| Hematology | 8 (2.7%) |
| Hepatobiliary | 41(13.7%) |
| Lung | 35 (11.6%) |
| Prostate | 15 (5.0%) |
| Sarcoma | 8 (2.7%) |
| Other | 15 (5.0%) |
Also, the most common prevalent symptoms among all patients in descending order were wellbeing (90%), pain (86%), fatigue (75%), anxiety (59%), and anorexia (55%). Depression was present in 41% of patients, nausea and vomiting (26%) and dyspnea (24%) (Table 2).
Table 2. Patients’ Symptom Prevalence
| Symptom Prevalence | N (%) | 95% Confidence Interval |
|---|---|---|
| Pain | 259 (86.3%) | (0.824 0.902) |
| Tiredness | 220 (74.8%) | (0.699 0.798) |
| Drowsiness | 98 (33.1%) | (0.277 0.385) |
| Nausea | 78 (26.3%) | (0.213 0.313) |
| Lack of Appetite | 164 (54.9%) | (0.492 0.605) |
| Shortness of Breath | 72 (24.2%) | (0.193 0.290) |
| Depression | 124 (41.3%) | (0.358 0.469) |
| Anxiety | 177 (59.2%) | (0.536 0.648) |
| Wellbeing | 265 (90.4%) | (0.871 0.938) |
Comparing the severity of symptoms. Pain and reduce general wellbeing scored the most severe symptoms among out-patients cancer patients in this study, 46.7% and 28% respectfully. While drowsiness (4.3%), nausea (3.4%), and shortness of breath (4.7%) were reported as the least severe symptoms among participants (Figure 1).
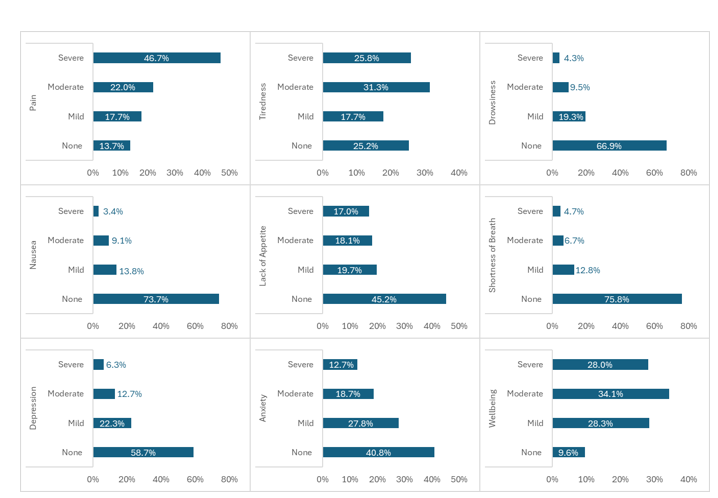
Figure 1:Symptom Severity
In addition, patients were divided in terms of symptom distribution into two subgroups according to age (as shown in Table 3). Those < 65 years of age and those ≥ 65 years. The highest reported symptom was reduce wellbeing (91%) among those ≥ 65 years. Also, it was found that pain was higher in patients < 65 years compared to older patients (88% versus 82%) as well as fatigue (75% versus 72%), anxiety (60% versus 55%), depression (42% versus 38%), dyspnea (25% versus 22%), and nausea (28% versus 20%). However, those differences in symptom prevalence between the two age groups were not statistically significant.
Table 3. Symptom distribution by age group
| Factor | <65 yrs | ≥65yrs | p-value |
|---|---|---|---|
| Total n=300 | n=240 | n=60 | |
| Pain | 210 (87.5%) | 49 (81.6%) | 0.239 |
| Tiredness | 178 (75.4%) | 42 (72.4%) | 0.636 |
| Drowsiness | 76 (32.1%) | 22 (37.3%) | 0.446 |
| Nausea | 66 (27.9%) | 12 (20.0%) | 0.217 |
| Lack of Appetite | 128 (53.6%) | 36 (60.0%) | 0.370 |
| Shortness of Breath | 59 (24.8%) | 13 (21.7%) | 0.614 |
| Depression | 101 (42.1%) | 23 (38.3%) | 0.598 |
| Anxiety | 144 (60.2%) | 33 (55.0%) | 0.459 |
| Wellbeing | 211 (90.2%) | 54 (91.5%) | 0.752 |
Discussion
The present study clearly demonstrates that reducing well-being, pain, and fatigue are the most prevalent symptoms among cancer patients referred to the palliative care outpatient clinic and seen for the first time by the palliative care team. These findings are in accordance with most of the published literature on symptom prevalence among palliative care patients seen in the outpatient clinic setting [5-10]. It is also similar to previous findings on the topic of symptom prevalence among palliative care in-patients, who were completely transferred under palliative care [5].
In a retrospective cross-sectional study on 255 ambulatory care cancer patients attending the palliative care clinics at Princess Margaret Hospital in Canada, Rachel P. et al [6] reported that fatigue (77%), pain (75%) and anorexia (66%) were the three most prevalent symptoms. This was proved through median ESAS scores of 7, for fatigue; and 5 for both pain and anorexia. Another retrospective study of 400 patients referred to 3 palliative care centers in London, UK, reported that pain (64%), anorexia (34%), constipation (32%), fatigue (32%) and dyspnea (31%) were the most prevalent symptoms [6].
Symptom patterns among 77 terminal cancer patients selected from 537 consecutive patients admitted to the Palliative care unit of the National Taiwan University Hospital, revealed that fatigue, anorexia, pain and depression were the 4 most common prevalent symptoms [7].
In an interesting study on the correlation between symptom prevalence among palliative care outpatients and their time to death [8], using the ESAS tool, amongst the total of 198 cancer patients who visited the palliative care outpatient clinics, it was reported that symptoms most strongly associated with time to death in those patients were anorexia (p=0.001), drowsiness (p=0.006), dyspnea (p=0.009) and fatigue (p=0.01). There was no established association between anxiety and depression to the time of death. A recent article published in 2023 by Rafaqat and colleagues [9], from the Aga Khan University Hospital in Pakistan reported upon symptom prevalence among 78 patients seen in the palliative care clinic using the ESAS tool. Fatigue, pain, and anorexia had the highest ESAS initial score (5/10). Although there was significant reduction in the initial ESAS scores, after administering palliative care intervention, for pain and anorexia, a similar reduction was not evident for fatigue. Reduction in ESAS score was further observed in depression and anxiety, following the first palliative care outpatient visit.
The impact of an ambulatory palliative care clinic on symptoms and service outcomes in cancer patients has been clearly depicted by Rajvi S. et al [11]. Here, they reported on a total of 249 cancer patients who had attended an ambulatory palliative care clinic and were addressed for symptom prevalence. This was done using the symptom assessment scale over a period of 4 years. The highest prevalence was for fatigue (88%), followed by pain (76%), anorexia (75%), insomnia (71%), dyspnea (70%), mood disturbances (70%) and nausea (28%). There was evidence of a high symptom burden in those group of patients; and the initial visit to the outpatient palliative clinic followed by a follow up visit within 4 weeks led to significant improvement in insomnia (p<0.001), pain (p=0.002), overall wellbeing (p<0.001) as well as overall symptom composite scores (p=0.028). The study also concluded that the comprehensive assessment of symptom prevalence and severity would improve those symptoms through early ambulatory palliative care clinic intervention.
It is worth noting that both anxiety and depression prevalence were higher (59% and 41% respectively) among our cohort of palliative care outpatients compared to the international figures recently updated in the American Society of Clinical Oncology publication in 2023 concerning anxiety and depression prevalence among patients with advanced cancer diagnoses; [12] which were reported to be between 20%-25%. This higher prevalence among our patients might be attributed to the fact that our population consists of a high percentage of expatriates who are single, with no family support, no psychological support [4]. In fact, we previously had reported a high percentage of psychological distress (62%) among our cancer patients at different stages of the disease as published in the British Journal of Cancer Research [10].
Also, in this study wellbeing was the most prevalent reported symptom with a percentage of 90%. This is consistent with a published study indicating that psychological symptoms are highly prevalent; with significant distress observed in 31% of patients which highlights the critical need to assess and support individuals living with cancer and to ensure the availability of counseling and psychological services [2].
As regards cancer type, the most common encountered malignancies in the present study were breast cancer (20.7%), Gastrointestinal cancers (20.3%), Hepatobiliary cancer (13.7%), Lung (11.6%) and gynecological cancers (11.3%). This distribution is in accordance with the most common cancer types reported in a group of 301 palliative care patients at St. Paul Hospital, Ethiopia [13], where gynecological and breast cancers were the most common cancer types with an incidence of 25.9% and 16.9% respectively. The incidence of lung cancer in the above-mentioned study was also similar to that observed in our study (10.6% and 11.6% respectively).
The distribution of the most common cancer types is however different from recent published studies. For instance, an Italian study performed in 2023 [14] where Genitourinary cancers (26%), followed by Gastrointestinal (20.8%), lung (18.2%) and breast (14%) cancers were the most commonly frequent cancer types.
In a large retrospective study from MD Anderson Cancer Center including 406 patients seen for the first time in the palliative care outpatient clinics, [15] Lung cancer followed by Head and neck cancers were the most frequent cancer types (29%), preceding gastrointestinal (17%), genitourinary (14%), breast (11%), and gynecological cancers (7%).
The only study from our region of the Arabian Peninsula, was published in 2012 from Saudi Arabia [16] where they reported breast cancer (27.4%), head and neck (15.3%), genitourinary (12.9%), gastrointestinal (9.7%), and gynecological cancers (9.7%) as the most frequent cancer types among 124 patients. Those patients too were referred to palliative care outpatient clinics for the first time.
There was no association between age groups (<65 years versus ≥ 65 years) and symptom prevalence in the present study. This is contrasting previous results of a study on palliative care inpatients completely transferred under palliative care; where younger patients (<65 years) had statistically significantly higher prevalence of pain, anorexia, depression, and anxiety [5].
In addition, in the study of Abdullah et al. [5] of 400 palliative care in NCCCR [4], all symptoms were significantly higher among inpatients compared to those of 300 outpatient’s cohort. Fatigue, drowsiness, nausea, anorexia, dyspnea, depression, and anxiety, except for pain which was slightly higher (86%) in outpatients versus inpatients (84%). The overall wellbeing of palliative care inpatients was more affected (98.2%) as compared to palliative care outpatients (90.4%). This indicate these inpatients were referred late to palliative care services with an expected poorer performance status, which indicates that they are at the end of their life. Therefore, it is significantly recommended that earlier integration of palliative care for patients with advanced cancer diagnosis would undoubtedly result in a lower symptom burden and a better quality of life [1,9,11,17,18].
Conclusion
The present study demonstrates that wellbeing, pain, fatigue, anxiety, anorexia, and depression are the most common prevalent symptoms among palliative care outpatients attending the clinic for their first visit. When compared the severity of these symptoms, pain and reduce general wellbeing were scored the highest. Although, there were differences in symptoms prevalence among different age groups; this was not significantly different. In conclusion, the overall findings emphasizes the importance of earlier integration of palliative care for the overall management of patients diagnosed with advanced cancer.
Acknowledgment
The authors wish to express their sincere appreciation to Mostafa AbdelMaksound for his significant contribution to participants recruiting data collection, and support throughout the research process.
References
1. Phongtankuel V, Teresi JA, Eimicke JP, Kong JX, Adelman RD, et al. Identifying the prevalence and correlates of caregiver-reported symptoms in home hospice patients at the end of life. J Palliat Med. 2020;23(5):635-40.
2. Webber K, Davies AN, Leach C, Waghorn M. Symptom prevalence and severity in palliative cancer medicine. BMJ Support Palliat Care. 2023;13(Suppl 2):e270-2.
3. Hui D, Bruera E. The Edmonton Symptom Assessment System 25 years later: past, present, and future developments. J Pain Symptom Manage. 2017;53(3):630-43.
4. Shah R, Georgousopoulou EN, Al-Rubaie Z, Sulistio M, Tee H, Melia A, et al. Impact of ambulatory palliative care on symptoms and service outcomes in cancer patients: a retrospective cohort study. BMC Palliat Care. 2022;21(1):28.
5. Abdullah HM, Allam A, Alkeldi S, Idris Z, Hassan A. 1604P A comparative study of symptom prevalence between adults and elderly patients with advanced cancer diagnosis under palliative care: a single institution experience. Ann Oncol. 2023;34(Suppl 2):S889-90.
6. Riechelmann RP, Krzyzanowska MK, O’Carroll A, Zimmermann C. Symptom and medication profiles among cancer patients attending a palliative care clinic. Support Care Cancer. 2007;15(12):1407-12.
7. Potter J, Hami F, Bryan T, Quigley C. Symptoms in 400 patients referred to palliative care services: prevalence and patterns. Palliat Med. 2003;17(4):310-4.
8. Tsai JS, Wu CH, Chiu TY, Hu WY, Chen CY. Symptom patterns of advanced cancer patients in a palliative care unit. Palliat Med. 2006;20(6):617-22.
9. Cheung WY, Barmala N, Zarinehbaf S, Rodin G, Le LW, Zimmermann C. The association of physical and psychological symptom burden with time to death among palliative cancer outpatients. J Pain Symptom Manage. 2009;37(3):297-304.
10. Rafaqat W, Syed AR, Ahmed IM, Hashmi S, Jabeen I, Rajwani S, et al. Impact of an outpatient palliative care consultation and symptom clusters in terminal patients at a tertiary care center in Pakistan. BMC Palliat Care. 2023;22(1):75.
11. Hassan AA, Saleem AN, Eziada SJ, Bashir A, Gameil A, Elmalik H, et al. Psychosocial distress among cancer patients: a single institution experience at the state of Qatar. 2021.
12. Andersen BL, Lacchetti C, Ashing K, Berek JS, Berman BS, Bolte S, et al. Management of anxiety and depression in adult survivors of cancer: ASCO guideline update. J Clin Oncol. 2023;41(18):3426-33.
13. Amare N, Gintamo B, Tukeni KN, Gebremichael EH, Abera EG. The prevalence of cancer patients requiring palliative care and its associated factors at St. Paul Hospital, Addis Ababa, Ethiopia: a cross-sectional study. Risk Manag Healthc Policy. 2023;16:1203-14.
14. Bandieri E, Borelli E, Gilioli F, Bigi S, Mucciarini C, Ferrari U, et al. Stigma of palliative care among patients with advanced cancer and their caregivers on early palliative care. Cancers (Basel). 2023;15(14):3656.
15. Yennurajalingam S, Urbauer DL, Casper KLB, Reyes-Gibby CC, Chacko R, Poulter V, et al. Impact of a palliative care consultation team on cancer-related symptoms in advanced cancer patients referred to an outpatient supportive care clinic. J Pain Symptom Manage. 2011;41(1):49-56.
16. Al-Zahrani O, Eldali A, Al-Shahri MZ. Prevalence and severity of pain in cancer patients in an outpatient palliative care setting in Saudi Arabia. Qatar Med J. 2014;2014(1):6.
17. Zimmermann C, Swami N, Krzyzanowska M, Hannon B, Leighl N, Oza A, et al. Early palliative care for patients with advanced cancer: a cluster-randomised controlled trial. Lancet. 2014;383(9930):1721-30.
18. Lee YJ, Yang JH, Lee JW, Yoon J, Nah JR, Choi WS, et al. Association between the duration of palliative care service and survival in terminal cancer patients. Support Care Cancer. 2015;23(4):1057-62.
Received: August 04, 2025;
Accepted: September 26, 2025;
Published: September 30, 2025.
To cite this article : Allam A, Idris Z, Hassan A, Al Keldi S, Abdullah H, Jobran S, et al. Symptom prevalence among cancer patients attending the outpatient palliative care clinic: a single institutional experience. Br J Cancer Res. 2025;8(3):827-831. doi:10.31488/bjcr.211.
© The Author(s) 2025. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/).