Research article / Open Access
DOI: 10.31488/bjcr.206
The Drawing of Pain by Children and Adolescents with Cancer
Hilze Benigno de Oliveira Moura Siqueira,1; Amanda Batista Vilarindo2; Rodrigo Ramon Falconi Gomez3; Simone Saltareli4; Talita de Cassia Raminelli da Silva3; Fátima Aparecida Emm Faleiros Sousa2
1. Estácio IDOMED, Juazeiro-BA, Brazil
2. University of São Paulo, Brazil
3. Euro-American University Center, UNIEURO, Brazil
4. Paulista University, UNIP, Ribeirão Preto - SP, Brazil
*Corresponding author:Fátima Aparecida Emm Faleiros Sousa, Clinical Psychophysics Laboratory, University of São Paulo at Ribeirão Preto College of Nursing, Brazil, E-mail: ffaleiros@usp.br
Abstract
This study investigates the perception of pain in children and adolescents with cancer, using drawing and self-report as analysis tools. Recognizing pain as a multidimensional phenomenon - sensory, affective and cognitive -, the study proposes an expanded approach for its assessment in pediatric contexts. The research was conducted with 100 participants, aged between 5 and 18 years, treated at the Hospital das Clínicas de Ribeirão Preto between 2010 and 2012. The data were interpreted in light of Piaget and Luquet's theories of child graphic development, identifying three expressive stages: scribble (emphasis on the sensory dimension), intellectual realism (emphasis on the affective dimension) and visual realism (emphasis on the cognitive dimension). The drawings and verbal reports revealed symbolic representations of pain, often personified or metaphorized as “animals”, “darkness” or “balls of pain”. In addition to the location of the pain, participants expressed feelings such as fear, sadness, and helplessness. Younger children showed a more concrete understanding of pain, while adolescents demonstrated a greater capacity for abstraction and reflection. It was also observed that cancer can compromise cognitive development, indicating the need for interdisciplinary intervention, especially psychological support. It was concluded that the use of symbolic languages, such as drawing, combined with sensitive and qualified listening, constitutes a fundamental strategy for the humane and ethical management of pain in pediatric cancer patients. This approach contributes significantly to improving the quality of life and comprehensive care for children and adolescents with cancer.
Keywords: Pain, cancer, child, adolescent, famíly, development
Introduction
The concept of pain reveals an association with human suffering and recognizes, in itself, not only the sensory dimension, but also the psychological and social aspects involved. This multidimensional character of pain can be perceived in different phases of the human life cycle and existential experiences, which requires an appropriate assessment or measurement, according to the reality of each one [1,2].
Pain is an experience present in children and adolescents of all ages, being influenced by sensory, physiological, cognitive, emotional, behavioral and cultural factors. Emotions, beliefs and attitudes can modify its perception and transmission to the brain, impacting the way it is experienced and expressed [3].
Without proper assessment, pain may be misinterpreted or underestimated, which may lead to inadequate management and a reduction in the quality of life of those experiencing it. In the clinical setting, it is essential that this assessment be reliable in order to better plan pain management and achieve more effective management [3,4].
A study reveals that pain management in hospitalized children is still ineffective, indicating that, even with the implementation of a standardized pain assessment by institutions, this measure has not been fully sufficient or carried out in a complete manner. Understanding the profile of children with pain allows the multidisciplinary team to develop approaches that promote effective actions for pain relief, in a comprehensive and individualized manner. These approaches must consider each clinical specialty, recognize specific needs and integrate the subjectivity of the child, as well as their stage of development, ensuring a careful assessment that enables the creation of an individualized and humanized care plan [5].
Children and adolescents' responses to pain vary according to their age, stage of development, personality and environment, and can be expressed through behavior, facial expressions and verbalizations. To assess pain in different age groups and conditions, several scales can be used. In premature and full-term newborns, one example is the NIPS Scale (Neonatal Infant Pain Scale). For children under 4 years of age or unable to verbalize, the FLACC Scale (Face, Legs, Activity, Cry, Consolability) can be used as an alternative. From 4 years of age onwards, one option is the Wong-Baker Faces Scale, while children from 6 years of age can be assessed using the Visual Analogue Scale (VAS) and the Numeric Rating Scale (NRS). For children with disabilities or developmental difficulties, one possibility is the FLACC-R Scale (Face, Legs, Activity, Cry, Consolability – Revised). In adolescents, the APPT Scale (Adolescent Pediatric Pain Tool) can be used to assess acute or chronic pain. In addition to these scales, other tools such as the graphic technique – drawings can be applied according to the clinical need and the individual context of the child [6].
Through graphic means, children can express feelings, desires, fears and other aspects of their experiences. In view of this, several scholars have dedicated themselves to understanding this process of child expression, including Luquet and Lowenfeld. Based on the contributions of these authors, Piaget deepened the analysis of graphic means, associating it with cognitive development and the stages of the construction of children's thinking [7]. This assessment can be done by asking the child and/or their caregivers about pain, as well as by measuring it by health professionals themselves. Since isolated physiological parameters are not effective for this assessment, it should always be assessed using scales that have already been validated for the neonatal and/or pediatric age group and the condition of the patient in question [3]. In view of this, this study aimed to assess the perception of pain in children and adolescents with cancer, through drawing and self-report techniques.
Method
Study design
Descriptive exploratory study, using the drawing and self-report technique, addressing the propositions of Piaget [8,9] and Georges Henri Luquet [10].
Place and period
The research was carried out at the Hospital das Clínicas of the Faculty of Medicine of Ribeirão Preto of the University of São Paulo, in the outpatient clinic and in the oncopediatric sector of the Department of Childcare and Pediatrics specifically, from March 2010 to June 2012.
Participants
100 children and adolescents diagnosed with cancer, of both sexes, aged between 5 and 18 years old, participated in the study. Those who reported not having the physical conditions to perform the drawing task requested in the research were excluded.
Ethical aspects
The study was approved by the Research Ethics Committee of the Faculty of Medicine, under Process No. 3926/2009, using the Terms of Free Informed Consent (TCLE) and Free and Informed Assent (TALE), in addition to changing the names of the participants to those of precious stones, to guarantee the privacy and anonymity of each one.
Procedure
The research was carried out in 5 stages: 1. identification of participants from patient records; 2. collection of general information about pain and disease from medical records; 3. establishing rapport with participants; 4. certification of ethical research processes; 5. development of the research with the identification of pain perception mediated by the following guiding question: “If you could draw the pain you have ever felt or feel, what would you draw?”
It is important to emphasize that the instructions for the task were: 1) draw the pain, using the support materials provided, such as white A4 paper, colored pencils, crayons, No. 2 graphite pencils and felt-tip pens; 2) report on your perception and, 3) name the pain drawn.
Results
Pain was expressed through the drawing/story technique by 100 children and adolescents with cancer, in three different age groups, namely: 5-7 years (23%), 8-11 years (32%) and 12-18 years (45%), presenting some variations and uniformities in contours and meanings.
The results showed variations in relation to the presence of multiple dimensions of pain; sometimes with drawings linked to physical pain and illness, pain of a cognitive nature and, also, emotional pain. To better structure the results of this study, a random selection was implemented to choose and display the drawings, considering the dimension of pain, the characterization of the drawing and the development process in which the participants were, namely: 1) Drawing with expression of the sensitive dimension of pain and scribbled contours; 2) Drawing with the affective dimension of pain and contours of intellectual realism 3) Drawing with the cognitive dimension of pain and contours of visual realism.
1) Drawing with expression of the sensitive dimension of pain and scribble outlines
In Table 1, the drawings/reports by Alabastro and Barita show characteristics of the sensitive dimension and figures with scribbles.
Table 1:Drawings/reports of pain, referring to the graphic level of scribbles, of children with cancer, according to age, sex and Time of Diagnosis (TD) in months.
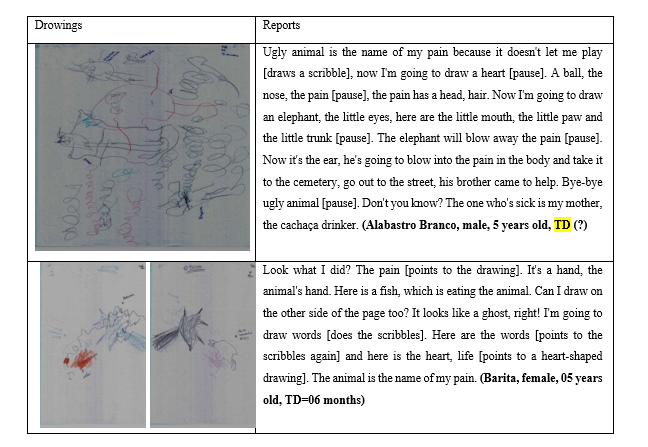
In the drawing by Alabatro, a 5-year-old boy, it is possible to identify a set of circular scribbles, with unrecognizable shapes, but with details that denote the sensitive dimension of pain in the expression of parts of the body (eyes, mouth, nose, head, etc.). This pain paralyzes his body and his games and is conceptualized as “ugly animal”. This indicates that in the painful experience of this child, the sensitive dimension is associated with the affective dimension.
In the case of Barita, a 5-year-old girl who had been diagnosed with cancer 6 months ago, she expresses the sensitive dimension of pain and shows the presence of scribbles in her doodles, without ordering the lines and without images of anything concrete. In addition, the report mentions a part of the body, the hand of an ‘animal’, which names her pain. In her doodles, Barita also draws scribbles, with little elaborate scribbles, but already using words and colors. This evocation of language and, mainly, of colors (“red colored heart”) does not yet seem to reveal the use of the secondary function of colors of a playful painting nature, but rather the representation of a part of the body associated with life (red colored heart).
2) Drawing with an affective dimension of pain and contours of intellectual realism
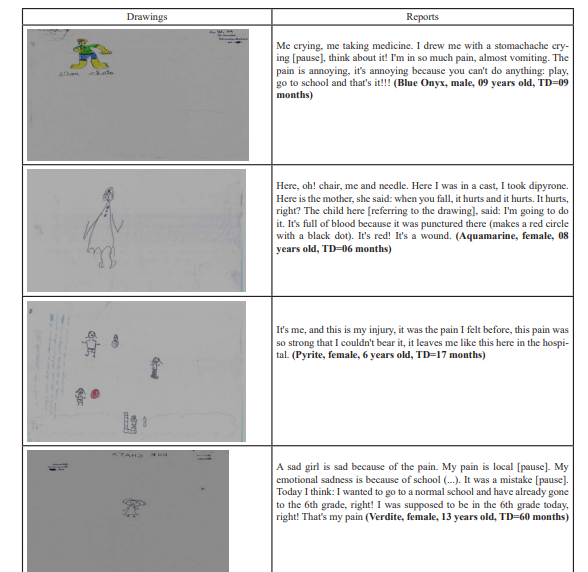
In Table 2, it was possible to observe drawings with the characteristics of the failed intellectual realism level proposed by Luquet [10] in which the child presents a graphic representation of space devoid of proportions, distances called Euclidean relations, as well as perspectives and directions of the set called projective relations associated with order, omissions, exaggerations, separations of drawn elements, elements of continuity and discontinuity of the parts of the object, according to the importance attributed by the child.
Table 2:Drawings/reports of pain, referring to the graphic level of synthetic disability, of children with cancer, according to age, sex and Time of Diagnosis (TD) in months
3)Drawing with cognitive dimension of pain and contours of visual realism
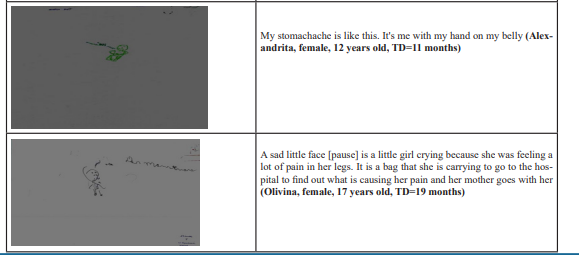
It consists of the drawing stage in which the aim is to reproduce the represented object, not only what can be seen, but everything that the person knows about it and what it is like. At this stage, there is a mixture of different points of view with elements of emphasis, transparency and planning, using perspective, opacity and overlapping to symbolize the object [10,11]. In Table 3, it is possible to identify the cognitive dimension and the drawing/report of pain regarding the graphic level of visual realism.
Table 3:Drawings/reports of pain referring to the graphic level of visual realism of children and adolescents with cancer, according to age, sex and Time of Diagnosis (TD) in months.
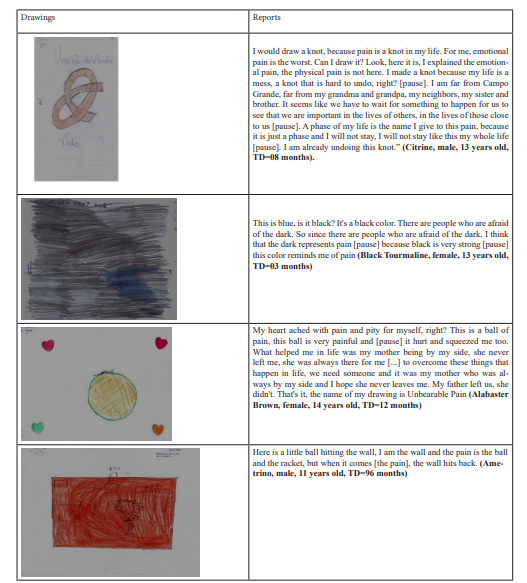
The results of the Table above show graphics referring to pain with varied symbolizations, namely: metaphorical figures (‘knot’, ‘darkness’, ‘ball and racket’, ‘balls in geometric shapes’); figures with elements that refer to therapeutic procedures and hospitalization (‘bandaged heart’, ‘syringe’, ‘serum and support’, ‘hospital bed’, ‘wall and building’).
Discussion
In the report of Alabastro's drawing in Table 1, this association or confluence is notable, as it evokes the memory of two parental models, the mother, with her behavior of supposed alcoholism that causes suffering ("the cachaça drinker") and the brother with emphasis on his behavior, which seems to bring her a feeling of help and protection.
Alabastro and Barita's report present movements and contours in their drawings, with perception of the body and interaction with the world around them, still characteristic of the features of the sensorimotor stage of development. However, it is not limited to this, since it vehemently expresses the pre-operational or symbolic phase, through the presence of the use of language and symbols to represent, imagine, classify and communicate what they think, know and feel [12].
In general, according to Luquet [10], graphic drawing reveals phases that accompany development, and are subdivided in this sequence: 1) scribbles, 2) intellectual realism and 3) visual realism. The Alabaster drawing seems to be close to the scribble phase, due to the characteristics of disordered scribbles. The sensitive dimension of pain can also be indicated when it describes parts of the body, integrated with figures of animals and memories of life experiences.
In terms of the dimension of pain, it was observed that children and adolescents thought of the painful phenomenon negatively, naming the pain as annoying and it was also associated with emotions, such as fear, sadness, longing, absence of family members, loss of the school environment, among others. The therapeutic management of hospitalization and hospitalization was perceived as a way of physical and emotional expression in this process, initially characterizing the subjective feeling of helplessness.
It was common to observe in Table 2, drawings containing human figures. Another characteristic found was the fact that the figures were organized on the paper without correct proportions and were more frequently small in size in the drawings.
Regarding the spatial disproportionality of the drawings, this was contrary to a study found in the literature [13] with drawings of the experiences of children and adolescents with cancer, which showed a tendency for drawings to contain contextual elements in medium and large sizes. For the authors, this data symbolizes a type of reaction to environmental pressure considered important (in adequate proportions) to the health-disease experience, and may also represent a certain aggressiveness, supposedly situational.
In a study carried out, when evaluating the drawings of children with cancer, some projective details of the drawings were brought up, among which is the use of drawings in small size, because when there is less frequency of the use of small size in the drawings, it is understood that this attribute provides positive indications of an attempt to overcome the pain and suffering caused by the illness [14].
Regarding the emphasis on the human figure in relation to its disproportionality on paper, a book on the pedagogy of children's drawing [15] highlights that from the age of six, in general, the child discovers the relationship between his/her drawing and reality, being able to represent the human figure, cognitively understand reality, the influence of culture and emotions. It is important to highlight that for Piaget [16], the ability that the child acquires to represent the human figure, the external world, is mediated by cognitive constructions or ways of thinking about models. Furthermore, this representation is presented in an increasing and consistent way. The progressive internalization of those actions that were performed in a sensorimotor way, in which intelligence is still practical, in the next phase, in addition to this practicality, the child begins to have intelligence in representation, which Piaget called pre-operational. This means that the child uses representation through assimilation, accommodation and balancing to organize these representations in a more integral way. And these operations mean exactly the capacity to organize this world of representations in a coherent and stable way, although it is not yet capable of reversing these operations, or of thinking in a direction opposite to that which was initially presented to it.
In general, it is possible to identify the graphic in terms of perceptive and cognitive spaces, however, unlike adults, children do not intend to narrate their pain, but to describe the experience in terms of order or nominal arrangement. This order in the drawing determines the learning of the relationship with places, sizes and even the omission of certain parts [17].
The emotional implications cannot be dissociated, so they will have elements of hospitalization, which can affect cognitive development, therefore requiring professional intervention, specifically from a psychologist to help improve the patient's well-being and quality of life and to provide pleasant memories of this scenario of illness [18].
In this universe, nothing is stagnant, but rather susceptible to transformations from one stage of development to another. We then discuss that, for example, when the child is in an age group below the expected graphic phase, there may be a need to understand the drawing as a whole, as well as the time of management of pain and illness. Therefore, we must not fail to consider that some of these children in an older age group, in pre-adolescence or adolescence, when they show that they are at a lower stage of cognitive development than expected, lead us to rethink the possibility of changes in the flow of their development due to the time of diagnosis of the disease.
The level of synthetic incapacity is striking in the graphic construction, also leading to negligence in the order of the drawing (tree and flowers in space, girl on top of the house), especially with the dispersion between parts and the whole of the page, which shows a lack of notion of the relations of distances and proportions of the illustrated elements and objects (girl bigger than the house, ruler bigger than the girl). The colors were also used without much coherence with reality. At this stage, the drawing still has a character of intended realism, however, this reality, in practice, has some flaws. Generally, because this reality begins at the moment when the child still does not know how to direct his/her graphic movements, his/her lines and colors do not look as intended [10,11]. In general, theories of human development, such as Piaget's, show man inserted in a relational web, whose determining and determining factor is associated with the responses and needs of the individual in relation to the environment in which he/she lives [11,19]. Such theories respect the inseparability of the dimensions of development, however they can study them separately.
In the diversity scenario in Table 3, the drawings/stories with metaphorical figures made by the pre-adolescents and adolescents Citrine, Black Tourmaline, Alabaster, Ametrine express that they have already been introduced to the perspective of thought, managing to have reasoning focused on visual realism in the face of the complexity of human pain. We can better exemplify this type of abstract reasoning learned through the drawing of the 'knot' presented by Citrine and the 'black color on paper' used by Black Tourmaline, which allows us to freely illustrate the fears, difficulties, and deprivations in the face of the dark existential world messed up by pain and cancer. The dark color used by Black Tourmaline was not used as a secondary, spontaneous and playful function as predicted by Luquet [10] and Piaget [20], but as a metaphor for meanings related to pain that may possibly be linked to the fear of darkness, ignorance or lack of clarification regarding the mystery surrounding being sick and the painful experience as a whole.
Metaphors (linguistic or visual) are considered “exchanges of thoughts”, open and ambiguous productions that refer one meaning to another. Metaphors propose surprising forms, including emotions, and do not provide answers. Children assimilate them from a young age, take them up again, and consider them a normal means of contact between people.
In a certain study [21], the world cannot be explained, nor can perceptions and emotions be transferred from one person to another. They can only be understood. Faced with this possibility, when pain for someone is defined as something dark, it is possible to borrow the ideas of Ferreira [22], who translates the term ‘dark’ as being the absence of light; something barely intelligible, hidden, mysterious; a monotonous, sad place; without luster, without shine. The idea and understanding brought about pain and the expression revealed by the drawing, in general, are correlated with the characteristics of development [11].
Piaget's research on how children and adolescents think describes the importance of considering the four stages he proposed (sensorimotor, pre-operational, concrete-operational and formal-operational) to understand whether development is occurring fluidly or not. With regard to this study, it is understood that the adolescents in Table 3 are in the hypothetical-deductive stage that begins around the age of 12 and is characterized by the ability to think about the relationships between events or between things and to think abstractly without having to actually experience them [23]. It is understood that drawings and stories are very important resources for understanding the processes in such a critical phase of life.
Conclusion
The use of the drawing technique accesses feelings, emotions and perceptions, allows for an approach that respects individuality and helps healthcare professionals identify the location, intensity and dimensions of pain.
Drawing encompasses important factors in an individual's life, from their experiences to their stimuli. Thus, we conclude that, for Piaget, drawing changes as development progresses, which is characterized by the person's experiences, considering that: "young children tend to ignore or transform reality into a subjective world, rich in fantasy. The analysis of drawings proved to be a valuable tool for accessing the sensitive, cognitive and affective existential dimensions of pain in children and adolescents with cancer. The lines, colors and shapes are representations loaded with meaning, which allow us to capture nuances of suffering that are often difficult to express verbally.
The use of this technique favors an individualized approach, respecting subjectivity and enabling healthcare professionals to identify fundamental aspects for a more comprehensive understanding of pain in its multiple facets.
This study reinforces the need for a thorough analysis of the painful phenomenon, allowing healthcare professionals to see the patient as a whole. This deeper understanding of the pain experience paves the way for more efficient management aligned with the specific needs of children and adolescents, strengthening the bond between the healthcare team, the patient and their family.
The cognitive dimension of pain is revealed as children and adolescents with cancer demonstrate, in their situational context, abilities to observe, identify, perceive, memorize, compare, classify, conceptualize, learn and draw conclusions from the painful experience.
Another relevant aspect is that the use of drawing, both as a form of expression and as a verbal record, contributes significantly to the analysis of pain perception at different stages of development. This resource reveals that, even from the age of 5, children are already capable of describing pain, although in a more categorical and concrete way, gradually evolving to more complex levels of abstraction.
Exploring the paths of pain and its universes implies a pact with the unknown, an immersion in the possible deviations of the flow of thought, perception and consciousness, laid bare in discourse. The way in which descriptors are captured, pain is represented and named is a process that is only possible through a deep dive into the interiority of the characters investigated — children and adolescents with cancer in their systemic web of family relationships.
This investigation led to reflections on the importance of understanding the sensitive, cognitive and affective dimensions present in pediatric oncology pain, paving the way for a more appropriate, humane and ethical management of pain in Brazilian public health. This process reveals the interaction of objective and subjective components that permeate the experience of children, adolescents and their families facing cancer and pain.
We understand that, when considering children or adolescents, their expressiveness and experience of pain and cancer emerge, bringing to light a condition submerged in the oscillations between health and illness, language and perception, and multifaceted pain, which involves an experience marked by history, affectivity and singularity.
This study is configured as a motivator for evaluations and measures in public health, in the areas of research and clinical practice, with the objective of promoting adequate management of pain during two crucial periods of the human life cycle: childhood and adolescence. Such periods, immersed in the family context and care, can be addressed in a palliative manner, ensuring that the end of life is lived with comfort, peace and dignity.
References
1. Raja SN, Carr DB, Cohen M, Finnerup NB, Flor H, Gibson S, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020 Sep;161(9):1976–82. doi: 10.1097/j.pain.0000000000001939.
2. Alcock MM. Defining pain: past, present, and future. Pain [Internet]. 2017 Apr [cited 2025 Jun 9];158(4):761–2.
3. Sociedade Brasileira de Pediatria. Dores comuns em pediatria: avaliação e abordagem. São Paulo: Departamento Científico de Medicina da Dor e Cuidados Paliativos da SBP; 2024.
4. Vilarindo AB, Sousa FAEF. Escala Multidimensional de Mensuração e de Avaliação de Dor (EMMADOR-SABER): percepção do conhecimento. 2022. [Type of publication not specified]
5. Carvalho JA, Souza DM, Flávia F, Amatuzzi E, Pinto MCM, Rossato LM. Pain management in hospitalized children: a cross-sectional study. Rev Esc Enferm USP. 2022;56:e20220008. doi: 10.1590/1980-220X-REEUSP-2022-0008en.
6. Abadesso C, coordinator. Desenhos da minha dor [Internet]. 1st ed. Lisboa: Círculo Médico; 2018 [cited 2025 Jun 9].
7. Santiago DE, Neto AF, Campos CFS, Batista MJR, Matuzaki PTT, Negrão TSF. O grafismo como representação do desenvolvimento do ser humano. Rev Cient Integr. 2020;4(5).
8. Piaget J. O juízo moral na criança. 3rd ed. São Paulo: Summus; 1994.
9. Piaget J. Seis estudos de psicologia. 24th ed. Rio de Janeiro: Forense Universitária; 1999.
10. Luquet GH. O desenho infantil. Porto: Editora do Minho; 1969.
11. Piaget J, Inhelder B. A psicologia da criança. 2nd ed. Rio de Janeiro: Bertrand Brasil; 2006. p. 114.
12. Piaget J. Seis estudos de Piaget. 25th ed. Rio de Janeiro: Forense Universitária; 2011.
13. Rezende AM, Brito VFDS, Malta J, et al. Vivências de crianças e adolescentes com câncer: o desenho fala. Iniciaç Cient CESUMAR. 2009;11(1):73–82.
14. Bacarji JEW, Gramacho PM. Desenhos de criança com câncer - uma avaliação da projeção. In: Nucci NAG, Perina EM, organizadores. As dimensões do cuidar em psiconcologia pediátrica. Campinas, SP: Livro Pleno; 2005. p. 77–111.
15. Sans PTC. A pedagogia do desenho infantil. 2nd ed. Campinas: Alínea; 2007.
16. Piaget J. O nascimento da inteligência na criança. 2nd ed. Rio de Janeiro: Zahar Editores; 1975.
17. Montoito F, Leivas JCP. A representação do espaço na criança, segundo Piaget: os processos mentais que a conduzem à formação da noção do espaço euclidiano. Vidya. 2012;32(2):21–35.
18. Rocha JR, De Araujo Mesquita D, Da Silva EP. O psicólogo atuando junto à criança hospitalizada. Cad Grad Ciênc Biol Saúde FITS. 2013;1(2):89–96.
19. Molinari JSO, Silva MFMC, Crepaldi MA. Saúde e desenvolvimento da criança: a família, os fatores de risco e as ações na atenção básica. Psicol Argum. 2005;23(43):17–26.
20. Piaget J. A linguagem e o pensamento da criança. 6th ed. São Paulo: Martins Fontes; 1993.
21. Staccioli G. As di-versões visíveis das imagens infantis. Pro-Posições. 2011 Aug;22(2):21–37.
22. Ferreira ABH. Dicionário da Língua Portuguesa. Rio de Janeiro: Positivo; 2010.
23. Piaget J. Epistemologia genética. São Paulo: Martins Fontes; 2002.
Received: February 17, 2025;
Accepted: March 18, 2025;
Published: March 20, 2025 .
To cite this article : Siqueira HBOM, Vilarindo AB, Gomez RRF, Saltareli S, da Silva TCR, Sousa FAEF. The Drawing of Pain by Children and Adolescents with Cancer. British Journal of Cancer Research. 2025; 8(2): 794- 801. doi: 10.31488/bjcr.206.
© The Author(s) 2025. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/).